Indications and Usage
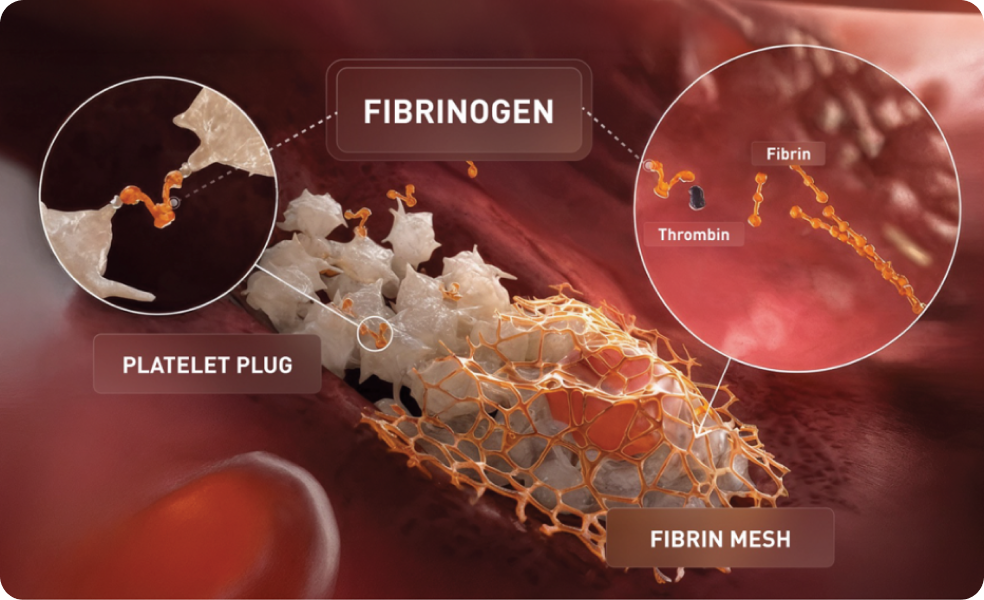
FESILTY (fibrinogen, human-chmt) is a human blood coagulation factor indicated for the treatment of acute bleeding episodes in pediatric and adult patients with congenital fibrinogen deficiency, including hypo- or afibrinogenemia.
Limitations of Use:
FESILTY is not indicated for dysfibrinogenemia.
Contraindications
FESILTY is contraindicated in patients who have severe hypersensitivity reactions, including anaphylaxis, to FESILTY or its components (arginine hydrochloride, polysorbate 80, sodium citrate dihydrate, trehalose dihydrate).
Warnings and Precautions
Hypersensitivity reactions have occurred in patients receiving FESILTY. Should symptoms occur, discontinue FESILTY and administer appropriate treatment.
Thrombotic events have occurred in patients receiving FESILTY. Weigh the benefits of administration versus the risks of thrombosis.
FESILTY is made from pooled human plasma and may carry the risk of transmitting infectious agents, e.g., viruses, the variant Creutzfeldt-Jakob disease (vCJD) agent and, theoretically, the Creutzfeldt-Jakob disease (CJD) agent.
Adverse Reactions
The most serious adverse reactions observed with FESILTY were thrombotic events, including portal vein thrombosis, deep vein thrombosis, and pain in extremity with clinically suspected thrombosis. One patient had an episode of epilepsy and died due to extradural hematoma 4 weeks after administration of FESILTY.
In a clinical study, the most common adverse reactions that occurred in >2% of patients receiving FESILTY were pain in extremity, back pain, hypersensitivity reactions, pyrexia, thrombosis, fibrin D dimer increased, headache, and vomiting.
Please see full Prescribing Information for FESILTY.
To report SUSPECTED ADVERSE REACTIONS, contact Grifols Therapeutics LLC at 1-800-520-2807 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.